

Abstract
Background
The role of self-antigen-targeting T cells is well established in multiple autoimmune disorders. In immune thrombocytopenia (ITP), CD8+ cytotoxic T cells target both peripheral blood platelets and bone marrow megakaryocytes. In addition, CD4+ helper T cell imbalance and cytokine secretion leads to the release of autoantibodies by B cells favoring the destruction of platelets. In order to understand if somatic mutations play a role and drive the aberrant immune responses in ITP, we analyzed sorted CD4+ and CD8+ T cells with deep sequencing panel.
Methods
The study population consisted of 13 adult patients diagnosed with chronic ITP (median age 47 years) at least one year before the first sampling. The median number of lines of therapy was 4, (range 0-8). In addition, 11 healthy control samples were collected for T cell phenotyping and TCR analysis (median age 63 years). After separation of peripheral blood mononuclear cells, immunophenotyping by flow cytometry was performed for CD4+ and CD8+ T cells and both fractions were sorted using magnetic beads. The CD4+ and CD8+ clonality was analyzed by deep sequencing of TCRB CDR3 using Adaptive platform. Custom-made deep sequencing gene panel covering 2433 genes related to immunity and cancer was used to analyze somatic mutations from 11 ITP patients. Mean target coverage was 567X (range 405-757X). Somatic variants with over 2% variant allele frequency (VAF) were called using Varscan2-based bioinformatics tool and CD4+ and CD8+ fractions were used as each other's germline control. Candidate somatic variants were visually validated with Integrative Genomics Viewer.
Results
ITP patients harbored clonal TCR rearrangements both in CD8+ and CD4+ fractions. The median percentage of the largest T cell clone of all TCR rearrangements in an individual sample was 9.5% (range 1.8%-31.9%) in CD8+ cells and 7.1% (range 0.9-13.6%) in CD4+. The median clone size or clonality index did not differ between ITP patients and healthy controls. Age correlated with the largest rearrangement and clonality index both in CD4+ and CD8+ fractions in ITP patients (r=0.70, p=0.015 and r=0.60, p=0.043 for CD4+ and r=0.63, p=0.033 and r=0.77, p=0.0050 for CD8+), but no correlation was observed in healthy controls.
The size of the maximum CD8+ TCR rearrangement and clonality index correlated positively with the percentage of highly cytotoxic CD8+CD57+ (r=0.80, p=0.0029 and r=0.90, p=0.0002) and terminally differentiated CD8+ effector memory with CD45RA (TEMRA) T cells (r=0.66, p=0.022 and r=0.78, p=0.0038). In healthy controls positive correlation was observed only between CD8+ clonality index and CD8+CD57+ T cells, but not with TEMRAs.
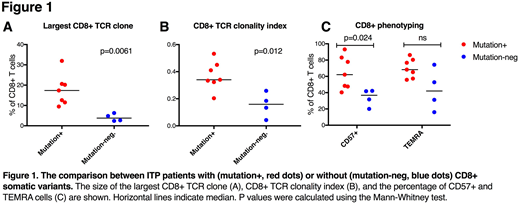
Somatic mutations in CD8+ T cells were detected in 7/11 (64%) of ITP patients. Somatic variants were distinct between individuals and their mean variant allele frequency (VAF) was 4.5% (range 2.0-13.6%). The mutated genes included those related to IFNg-signaling pathway (STAT1, NLRP4, CARD6, and EBF1), apoptosis (CASP6), and inflammation and cancer (ATM, EGR1, NOD1). ITP patients with CD8+ mutations had larger immunodominant CD8+ TCR clone (Figure 1A) and higher CD8+ clonality index (Figure 1B). The patients with CD8+ mutations had more cytotoxic CD8+CD57+ T cells than mutation-negative cases, but CD8+TEMRAs did not differ between the two groups (Figure 1C).
The mutation profile of the CD4+ samples was different: 3/11 (27%) of the ITP patients had mutations in the genes connected to clonal hematopoiesis of indeterminate potential (CHIP). One patient with a maximum of 8% clone in CD4+ T cells harbored mutations both in TET2 (VAF 13.5%) and PPM1D (VAF 12.8%): the VAFs suggest that the mutation was not restricted to the largest CD4+ clone. The second patient had a different mutation in PPM1D gene (VAF 2.8%) and the third one had a PPM1B-mutation both in CD4+ (VAF 18.0%) and CD8+ (VAF 11.1%) T cells.
Conclusions
To our knowledge, this is the first report of somatic variants in T cells in patients with ITP. Discovered somatic mutations in CD8+ T cells were associated with increased clonality and highly cytotoxic phenotype of CD8+ T cells. Interestingly, three patients harbored mutations in CHIP-associated genes in CD4+ and also in CD8+ fraction, with recurrent PPM1D-mutations. Further studies and screening of a larger ITP patient cohort is warranted to understand the meaning and functional consequence of somatic mutations in the pathogenesis of chronic ITP.
Ebeling:Boehringer Ingelheim: Consultancy; Celgene: Speakers Bureau; Otsuka Pharma Scandinavia AB: Consultancy. Mustjoki:Bristol-Myers Squibb: Honoraria, Research Funding; Novartis: Honoraria, Research Funding; Ariad: Research Funding; Celgene: Honoraria; Pfizer: Honoraria, Research Funding.

